
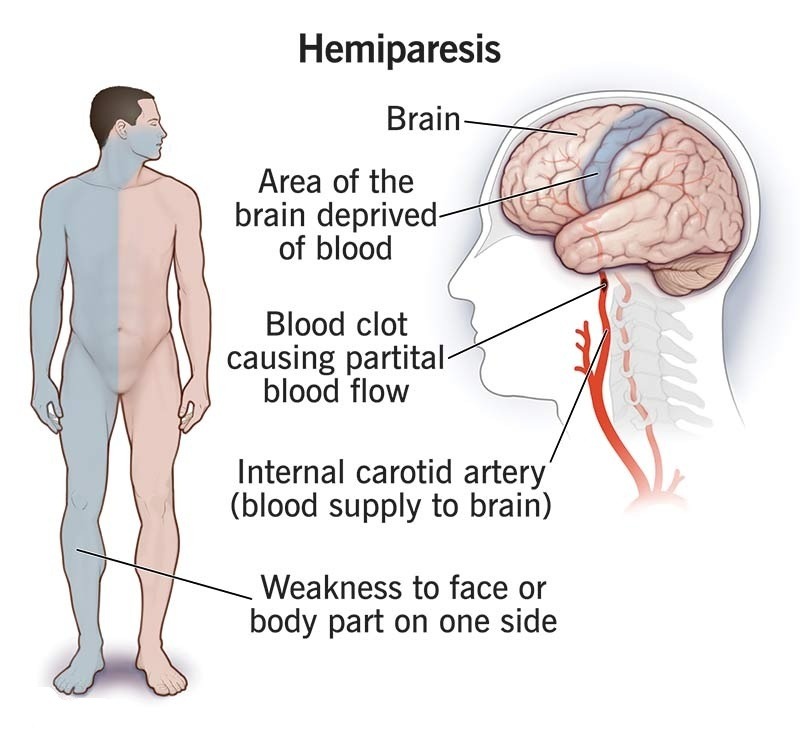
Hemiparesis – Overview
Hemiparesis is weakness affecting one side of the body (face, arm, leg, or a combination). It is a neurological symptom, not a disease itself, and indicates a problem in the brain, spinal cord, or peripheral nerves.
⚠️ Sudden-onset hemiparesis is a medical emergency and should be treated as a possible stroke until proven otherwise.
Key Clinical Features
One-sided muscle weakness
Reduced power compared to the opposite side
May involve face, upper limb, lower limb, or all three
Can occur with:
Speech difficulty
Facial droop
Vision changes
Balance or coordination problems
Why Hemiparesis Happens (Neuroanatomy Explained Simply)
Location of the problem: Side affected
Above decussation (brain): Opposite side (contralateral)
Below decussation (spinal cord/peripheral nerves): Same side (ipsilateral)
Cranial nerves (face/head): Usually same side
Decussation refers to the crossing of motor nerve fibers in the brainstem, which explains why brain lesions affect the opposite side of the body.
Common Causes of Hemiparesis
Vascular
Stroke (ischemic or hemorrhagic)
Transient Ischemic Attack (TIA)
Lacunar infarcts (small-vessel disease)
Brain aneurysm or hemorrhage
Traumatic
Traumatic brain injury (TBI)
Spinal cord injury+
Birth injury (e.g., cerebral palsy)
Neurological & Medical
Brain tumors
Multiple sclerosis (MS)
Seizures (post-ictal weakness)
Infections (encephalitis, meningitis)
Bell’s palsy (facial hemiparesis)
Hemiplegic migraine
Treatment of Hemiparesis
Treatment depends entirely on the underlying cause:
Cause type: Management approach
Stroke/TIA: Emergency care, thrombolysis, secondary prevention
Infection: Antivirals/antibiotics
Tumors: Surgery, radiotherapy, chemotherapy
MS/autoimmune: Immunomodulatory therapy
Permanent damage: Rehabilitation (physiotherapy, OT, neuro-rehab)
➡️ In cases of permanent CNS injury, strength may not fully return, but function can often improve with rehabilitation.
Risks of Not Treating Hemiparesis
Permanent brain damage
Paralysis
Loss of function
Disability
Death (in stroke cases)
What Is Ataxic Hemiparesis?
Ataxic hemiparesis is a combination of:
Weakness (hemiparesis)
Poor coordination (ataxia)
🔹 Most commonly caused by lacunar strokes affecting small blood vessels in the brain.
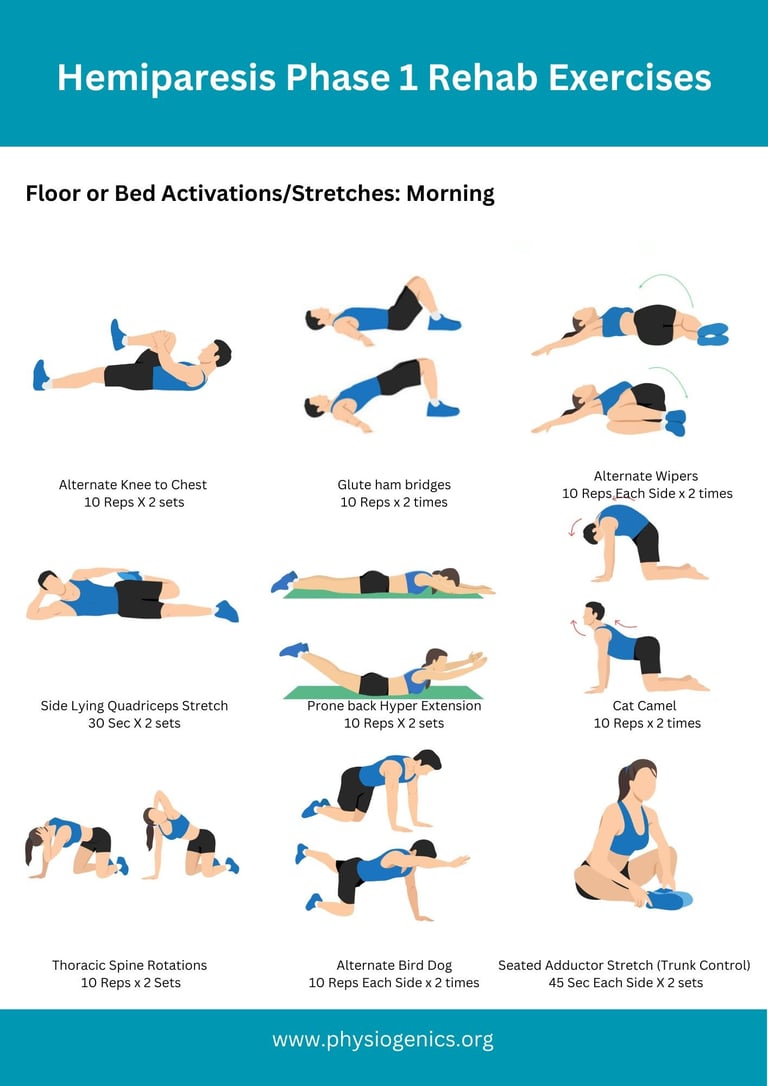
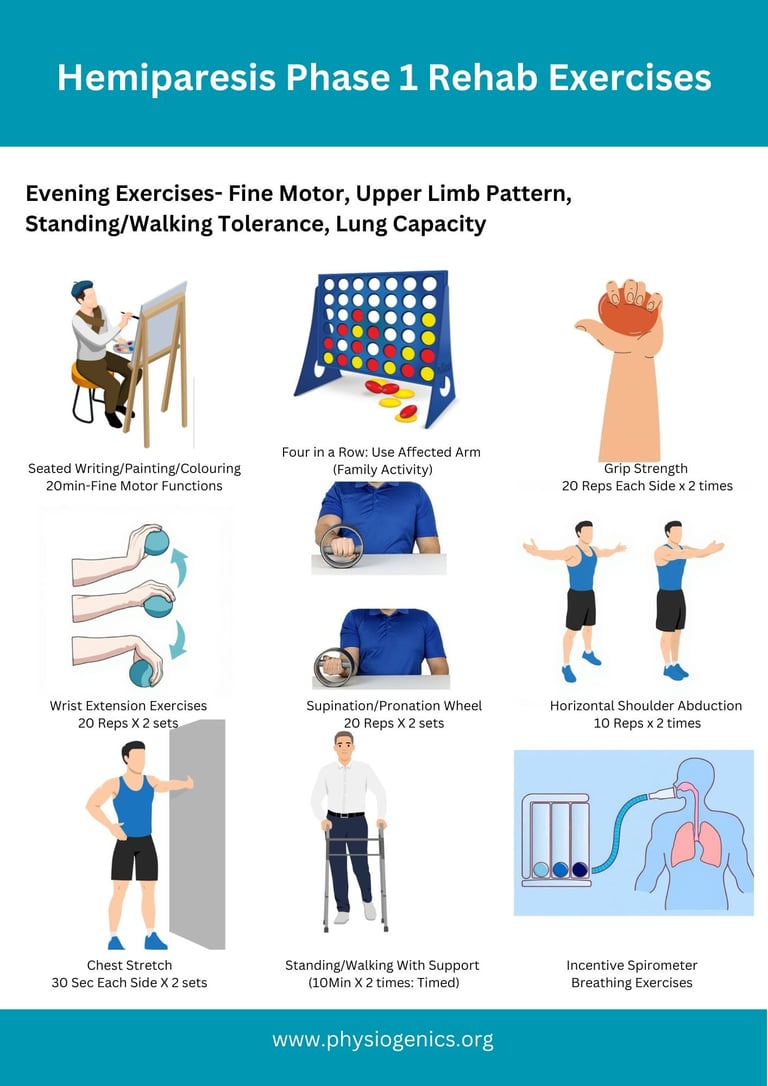
Goals of the Initial Phase (first 4-5 weeks)
Prevent joint stiffness, contractures, and shoulder subluxation
Maintain range of motion in all Upper & Lower Limb
Promote early activation of the affected side
Improve postural control and bed mobility
Prevent complications (pressure sores, chest infection, DVT)
Do’s
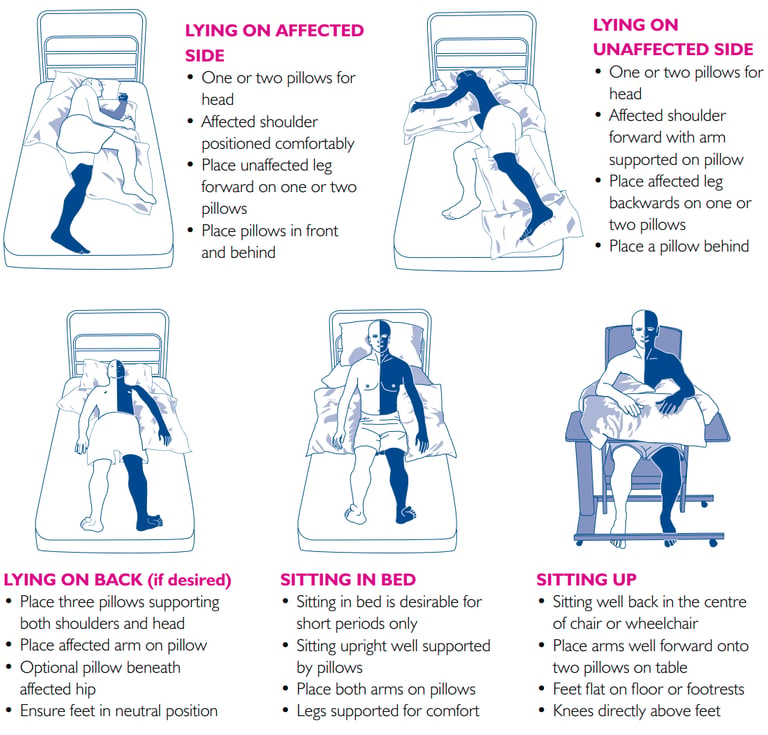
1. Positioning (VERY IMPORTANT)
2. Passive & Assisted Range of Motion (ROM)
Performed slowly, pain-free, 1–2 times/day.
Upper Limb
Shoulder flexion, abduction, external rotation
Elbow flexion/extension
Forearm pronation/supination
Wrist and finger extension (important to prevent flexor tightness)
Lower Limb
Hip flexion/extension, abduction
Knee flexion/extension
Ankle dorsiflexion/plantarflexion
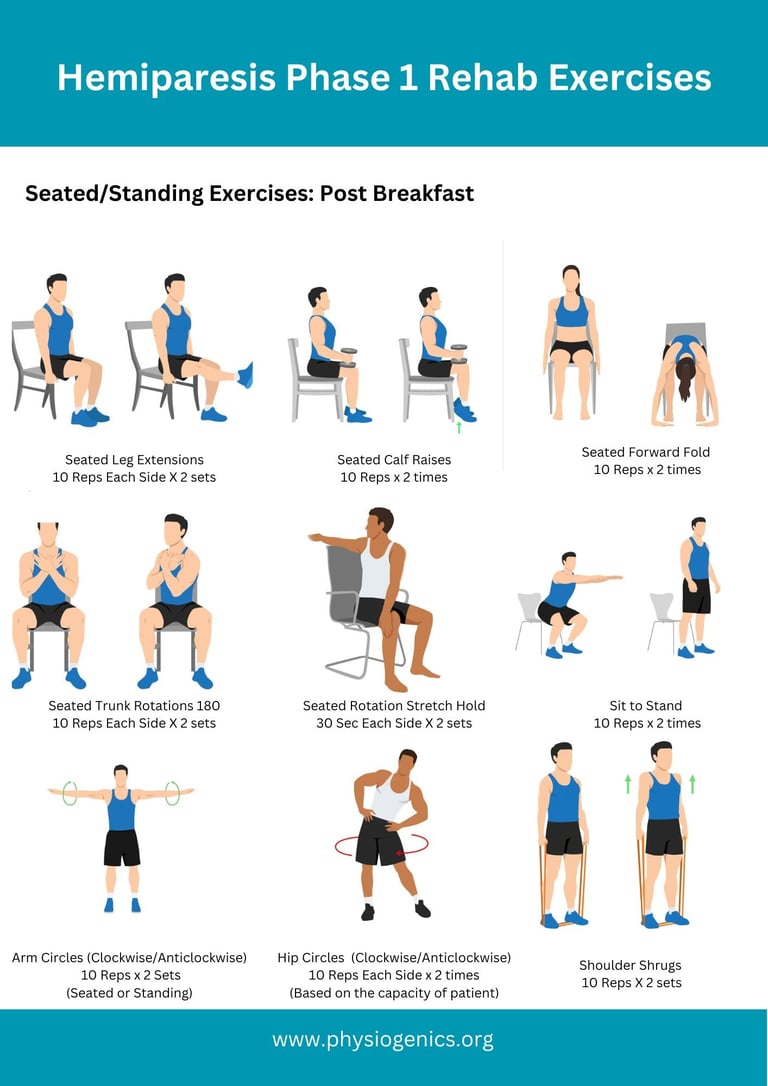
3. Early Active or Active-Assisted Exercises (as soon as possible)
In the early stage avoid resistance training
❌ DON’Ts
1. ❌ Do NOT Pull the Affected Arm
Never lift or turn the patient by the affected arm
Avoid pulling during transfers
➡ Can cause shoulder subluxation and pain
2. ❌ Avoid Forceful Stretching
No jerky or fast movements
No pushing into pain
➡ Can increase spasticity and cause injury
3. ❌ Do NOT Ignore the Affected Side
Don’t let the patient use only the strong side
Encourage looking at, touching, and moving the affected side
4. ❌ Avoid Prolonged Poor Positioning
No dangling arm unsupported
No prolonged wrist/finger flexion
No ankle left in plantarflexion (foot drop risk)
5. ❌ No Resistance Exercises Early On
Avoid weights or strong resistance
Especially if muscle tone is flaccid or just emerging
6. ❌ Don’t Over-Fatigue
Stop if:
Increased weakness
Dizziness
Excessive spasticity
Pain
Fatigue slows recovery.
Warning Signs – Stop and Seek Medical Advice
Sudden increase in weakness
Severe shoulder pain
New confusion or headache
Chest pain or breathlessness
Swelling or redness in leg (possible DVT)
Key Principles to Remember
Early, gentle, repetitive movement
Quality over quantity
Use the affected side safely
Consistency every day